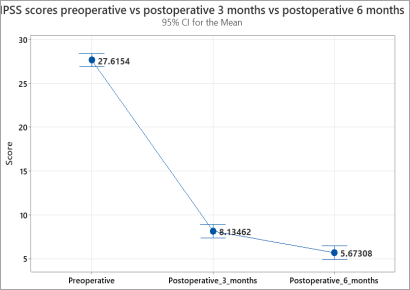
Background: Bladder outlet obstruction, common in older men, shows increased detrusor pressure and reduced urine flow during voiding. Diagnosis typically involves studying flow-rate and detrusor pressure values. Transvesical prostatectomy is a common treatment for significant prostatic enlargement, but real-world outcome data are scarce. Objective: To assess symptomatic improvement, changes in urinary incontinence and complications after transvesical prostatectomy for benign prostatic hyperplasia. Methods: Prospective cross-sectional study design was used and SPSS statistical software version 25 was used for data entry and analysis. Results: The mean age of patients with benign prostatic hyperplasia was 64.73±8.7 years. Preoperative international prostate symptoms score (IPSS) was 27.6±3.08. At 3 months, IPSS declined significantly to 8.13±2.86 (p<0.001). Preoperative incontinence completely resolved in 30% and partially improved in 70% of patients. New onset incontinence occurred in 13.5%. At 6 months, IPSS was 5.67±2.31. Of those with new postoperative incontinence, 42.9% completely resolved and 57.1% improved. For preoperative incontinence, 71.4% completely resolved and 28.6% partially improved. Erectile function failed to improve. Conclusion: The study showed trans-vesical prostatectomy results promising results in lower urinary tract symptoms improvement. Post-op incontinence got better for most, but erectile function didn't return to normal.
| Published in | Science Journal of Clinical Medicine (Volume 13, Issue 2) |
| DOI | 10.11648/j.sjcm.20241302.11 |
| Page(s) | 21-28 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Benign Prostatic Hyperplasia, Bladder Outlet Obstruction, Trans-Vesical Prostatectomy
2.1. Study Area and Period
2.2. Study Design
2.3. Source and Study Population
2.4. Inclusion and Exclusion Criteria
2.5. Study Variables
2.6. Data Collection Technique and Quality Control
2.7. Data Processing and Analysis
3.1. Demographic Characteristics of Participants
3.2. Causes of Bladder Outlet Obstruction and Type of Surgery
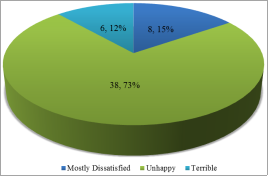
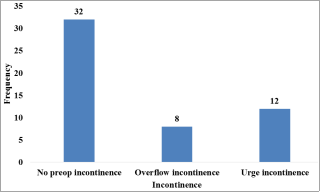
3.3. Preoperative Symptoms and Bother Scores
3.4. Postoperative Outcomes at 3 Months
Bother Score | Frequency | Percent |
|---|---|---|
Delighted | 2 | 3.80% |
Pleased | 22 | 42.30% |
Mostly satisfied | 22 | 42.30% |
Mixed (About Equally Satisfied and Dissatisfied) | 4 | 7.70% |
Mostly Dissatisfied | 2 | 3.80% |
Incontinence status | Frequency | Percent |
|---|---|---|
New onset postoperative incontinence | 7 | 13.5% |
Preoperative incontinence (n=20) | ||
Completely resolved | 6 | 30% |
Partially improved | 14 | 70% |
3.5. Postoperative Outcomes at 6 Months
Bother Score | Frequency | Percent |
|---|---|---|
Delighted | 19 | 36.5 |
Pleased | 22 | 42.3 |
Mostly satisfied | 9 | 17.3 |
Mixed (About Equally Satisfied and Dissatisfied) | 2 | 3.8 |
3.6. Postoperative Outcomes Based on Age and Occupation
| [1] | Parsons, J. K., Benign prostatic hyperplasia and male lower urinary tract symptoms: epidemiology and risk factors. Current bladder dysfunction reports, 2010. 5: p. 212-218. |
| [2] | Berry, S. J., et al., The development of human benign prostatic hyperplasia with age. The Journal of urology, 1984. 132(3): p. 474-479. |
| [3] | McVary, K. T., et al., Update on AUA guideline on the management of benign prostatic hyperplasia. The Journal of urology, 2011. 185(5): p. 1793-1803. |
| [4] | Lose, G., et al., Standardisation of urethral pressure measurement: report from the Standardisation Sub-Committee of the International Continence Society. Neurourology and Urodynamics: Official Journal of the International Continence Society, 2002. 21(3): p. 258-260. |
| [5] | Martin, S. A., et al., Prevalence and factors associated with uncomplicated storage and voiding lower urinary tract symptoms in community-dwelling Australian men. World journal of urology, 2011. 29: p. 179-184. |
| [6] | Agarwal, A., et al., What is the most bothersome lower urinary tract symptom? Individual-and population-level perspectives for both men and women. European urology, 2014. 65(6): p. 1211-1217. |
| [7] | Ahyai, S. A., et al., Meta-analysis of functional outcomes and complications following transurethral procedures for lower urinary tract symptoms resulting from benign prostatic enlargement. European urology, 2010. 58(3): p. 384-397. |
| [8] | Cornu, J.-N., et al., A systematic review and meta-analysis of functional outcomes and complications following transurethral procedures for lower urinary tract symptoms resulting from benign prostatic obstruction: an update. European urology, 2015. 67(6): p. 1066-1096. |
| [9] | Lucca, I., et al., Outcomes of minimally invasive simple prostatectomy for benign prostatic hyperplasia: a systematic review and meta-analysis. World journal of urology, 2015. 33: p. 563-570. |
| [10] | Burke, N., et al., Systematic review and meta-analysis of transurethral resection of the prostate versus minimally invasive procedures for the treatment of benign prostatic obstruction. Urology, 2010. 75(5): p. 1015-1022. |
| [11] | Rassweiler, J., et al., Complications of transurethral resection of the prostate (TURP)—incidence, management, and prevention. European urology, 2006. 50(5): p. 969-980. |
| [12] | Mamoulakis, C., D. T. Ubbink, and J. J. de La Rosette, Bipolar versus monopolar transurethral resection of the prostate: a systematic review and meta-analysis of randomized controlled trials. European urology, 2009. 56(5): p. 798-809. |
| [13] | Mebust, W., et al., Transurethral prostatectomy: immediate and postoperative complications. A cooperative study of 13 participating institutions evaluating 3,885 patients. The Journal of urology, 1989. 141(2): p. 243-247. |
| [14] | Fasciolo, A. and C. Baldini, Transvesical prostatic adenomectomy: general or local anesthesia. Urologia Journal, 2008. 75(4): p. 221-227. |
| [15] | Irwin, D. E., et al., Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. European urology, 2006. 50(6): p. 1306-1315. |
| [16] | Coyne, K. S., et al., The prevalence of lower urinary tract symptoms (LUTS) in the USA, the UK and Sweden: results from the Epidemiology of LUTS (EpiLUTS) study. BJU international, 2009. 104(3): p. 352-360. |
| [17] | Tkocz, M. and A. Prajsner, Comparison of long-term results of transurethral incision of the prostate with transurethral resection of the prostate, in patients with benign prostatic hypertrophy. Neurourology and Urodynamics: Official Journal of the International Continence Society, 2002. 21(2): p. 112-116. |
| [18] | Reich, O., C. Gratzke, and C. G. Stief, Techniques and long-term results of surgical procedures for BPH. European urology, 2006. 49(6): p. 970-978. |
| [19] | Thomas, A. W., et al., The natural history of lower urinary tract dysfunction in men: minimum 10-year urodynamic followup of transurethral resection of prostate for bladder outlet obstruction. The Journal of urology, 2005. 174(5): p. 1887-1891. |
| [20] | Parry, M. G., et al., Urinary incontinence and use of incontinence surgery after radical prostatectomy: a national study using patient‐reported outcomes. BJU international, 2022. 130(1): p. 84-91. |
| [21] | Elshal, A. M., H. M. Elmansy, and M. M. Elhilali, Transurethral laser surgery for benign prostate hyperplasia in octogenarians: safety and outcomes. Urology, 2013. 81(3): p. 634-639. |
| [22] | Lokeshwar, S. D., et al., Epidemiology and treatment modalities for the management of benign prostatic hyperplasia. Translational andrology and urology, 2019. 8(5): p. 529. |
APA Style
Gebremichael, N., Abdissa, M., Amtataw, W., Endazenaw, G. (2024). Surgical Management Outcome of Benign Prostatic Hyperplasia in Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia. Science Journal of Clinical Medicine, 13(2), 21-28. https://doi.org/10.11648/j.sjcm.20241302.11
ACS Style
Gebremichael, N.; Abdissa, M.; Amtataw, W.; Endazenaw, G. Surgical Management Outcome of Benign Prostatic Hyperplasia in Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia. Sci. J. Clin. Med. 2024, 13(2), 21-28. doi: 10.11648/j.sjcm.20241302.11
AMA Style
Gebremichael N, Abdissa M, Amtataw W, Endazenaw G. Surgical Management Outcome of Benign Prostatic Hyperplasia in Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia. Sci J Clin Med. 2024;13(2):21-28. doi: 10.11648/j.sjcm.20241302.11
@article{10.11648/j.sjcm.20241302.11,
author = {Niyat Gebremichael and Michael Abdissa and Wondwossen Amtataw and Getabalew Endazenaw},
title = {Surgical Management Outcome of Benign Prostatic Hyperplasia in Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia
},
journal = {Science Journal of Clinical Medicine},
volume = {13},
number = {2},
pages = {21-28},
doi = {10.11648/j.sjcm.20241302.11},
url = {https://doi.org/10.11648/j.sjcm.20241302.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjcm.20241302.11},
abstract = {Background: Bladder outlet obstruction, common in older men, shows increased detrusor pressure and reduced urine flow during voiding. Diagnosis typically involves studying flow-rate and detrusor pressure values. Transvesical prostatectomy is a common treatment for significant prostatic enlargement, but real-world outcome data are scarce. Objective: To assess symptomatic improvement, changes in urinary incontinence and complications after transvesical prostatectomy for benign prostatic hyperplasia. Methods: Prospective cross-sectional study design was used and SPSS statistical software version 25 was used for data entry and analysis. Results: The mean age of patients with benign prostatic hyperplasia was 64.73±8.7 years. Preoperative international prostate symptoms score (IPSS) was 27.6±3.08. At 3 months, IPSS declined significantly to 8.13±2.86 (pConclusion: The study showed trans-vesical prostatectomy results promising results in lower urinary tract symptoms improvement. Post-op incontinence got better for most, but erectile function didn't return to normal.
},
year = {2024}
}
TY - JOUR T1 - Surgical Management Outcome of Benign Prostatic Hyperplasia in Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia AU - Niyat Gebremichael AU - Michael Abdissa AU - Wondwossen Amtataw AU - Getabalew Endazenaw Y1 - 2024/04/17 PY - 2024 N1 - https://doi.org/10.11648/j.sjcm.20241302.11 DO - 10.11648/j.sjcm.20241302.11 T2 - Science Journal of Clinical Medicine JF - Science Journal of Clinical Medicine JO - Science Journal of Clinical Medicine SP - 21 EP - 28 PB - Science Publishing Group SN - 2327-2732 UR - https://doi.org/10.11648/j.sjcm.20241302.11 AB - Background: Bladder outlet obstruction, common in older men, shows increased detrusor pressure and reduced urine flow during voiding. Diagnosis typically involves studying flow-rate and detrusor pressure values. Transvesical prostatectomy is a common treatment for significant prostatic enlargement, but real-world outcome data are scarce. Objective: To assess symptomatic improvement, changes in urinary incontinence and complications after transvesical prostatectomy for benign prostatic hyperplasia. Methods: Prospective cross-sectional study design was used and SPSS statistical software version 25 was used for data entry and analysis. Results: The mean age of patients with benign prostatic hyperplasia was 64.73±8.7 years. Preoperative international prostate symptoms score (IPSS) was 27.6±3.08. At 3 months, IPSS declined significantly to 8.13±2.86 (pConclusion: The study showed trans-vesical prostatectomy results promising results in lower urinary tract symptoms improvement. Post-op incontinence got better for most, but erectile function didn't return to normal. VL - 13 IS - 2 ER -
Department of Surgery, Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia
Department of Surgery, Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia
Department of Surgery, Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia
Department of Public Health, Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia